
COVID (Mis-)Punditry with Dr. Marty Makary
Bari Weiss hosts a non-expert for a discussion about the pandemic.


I’m a fan of Bari Weiss. I read and listen to everything she produces. I find her to be a savvy observer of media bias and a thought-provoking writer. I tend to agree with the majority of her takes, but it’s the points of disagreement that I enjoy most since they always give me something to think about.
Her work resonates with me in the same way I find myself drawn to the likes of Matt Taibi, Glenn Greenwald, Joe Rogan, Sam Harris, and Ben Hunt, to name a few. Their collective willingness to call bullshit on what Eric Weinstein refers to as the gated institutional narrative is what appeals to me most. This crew’s work represents a certain heterodoxy that I appreciate.
Ms. Weiss hosts a podcast called Honestly with Bari Weiss. As a loyal listener, I took in a recent episode featuring Dr. Marty Makary entitled Is Covid…Over? And Other Burning Questions This Thanksgiving.
I had never heard of Dr. Makary before Ms. Weiss introduced him to me, but the man piqued my curiosity enough to warrant this writeup. More to the point, his comments struck me as some combination of hyperbolic and unrealistic over the course of their discussion. And while I wouldn’t expect Ms. Weiss to continuously challenge him along the way (she’s not a medical professional and hosts tend to be docile with their guests anyway), the lack of even subtle pushback was disappointing.
Before proceeding, I should confess my own priors up front. Firstly, and importantly(!), I’m not a doctor of any sort. I also don’t enjoy watching medical dramas on TV nor did I stay at a Holiday Inn last night, so I’d fail miserably at attempting even armchair expertise with any medical topic. The issues I highlight below are purely a function of my own curiosity and halfway decent understanding of risk.
Second, I try my best to consume information as objectively as I can. As we all do, I still bring my own biases to issues, but I try to pursue the type of independent open-mindedness that I admire in folks like Ms. Weiss. One bias I am fully aware of is that I really enjoy a good counter-narrative. I also share a mistrust in institutions that has driven a lot of the policy skepticism we see today. When it comes to most things establishment, I generally share Mr. Hunt’s BITFD sentiment. And I too really want to see our world return to normal as quickly as possible. All of this is to say that I was predisposed to enjoy this type of discussion.
Lastly, I have loosely held opinions on masks, vaccines, and COVID-related policy initiatives. I view masks as a minor annoyance with probably limited impact and vaccines as a gift of modern medicine. I think vaccine mandates are a bad idea, both in terms of overreach and in hardening opposition. I think certain cities/states/countries have been unnecessarily draconian in their crackdown attempts. I am sympathetic to the view that our leadership has not covered itself in glory during this ordeal, which if we’re being honest it rarely does. I attribute our policy clumsiness to rapidly evolving circumstances and poorly-constructed incentives rather than nefarious plots aimed at exerting control over the populace. When watching our leaders stumble their way through all this, I am reminded of a quote, “Never ascribe to malice that which is adequately explained by incompetence.”
The structure of this piece is mostly comprised of direct quotes of Dr. Makary from his discussion with Ms. Weiss, which are followed by my own commentary in response.
I will talk to doctors who are supposed experts…and that term is a very loose term because it’s usually a term crowned by the media.
This quote was pulled from about halfway through and nicely sets the stage for this piece. Invited onto this podcast to speak on the topic of the pandemic, Dr. Makary himself is not an epidemiologist or infectious disease expert. He is a Professor of Surgery at the Johns Hopkins School of Medicine. Per the school’s website, none of the dozens of topics listed under his Expertise and Research Interests pertain to the study of airborne pathogens.
This is a good example of the cognitive dissonance we so often see these days. Here is an accomplished surgeon and author with no apparent expertise in infectious diseases speaking with authority on the topic of COVID and its associated prophylactics and therapeutics. The irony of him being featured as an expert in light of this quote is rather rich.
Despite his lack of expertise, Dr. Makary has nonetheless become a bit of a talking head on COVID, making him precisely the media-crowned expert he dismisses here. A YouTube search finds dozens of videos of him waxing philosophical on COVID policy across platforms large and small. Funnily, he complains to Ms. Weiss about the media having their go-to experts to perpetuate some sort of narrative around vaccines, yet he too has become a go-to “expert” for those outlets seeking a counter-narrative.

The good doctor seems to enjoy the spotlight, perhaps due in part to the fact that he has a new book out. He writes and talks a lot, so his desire to feed the publicity machine is clear. The bio on his own website leads with the fact that he was the recipient of the Business Book of the Year Award in 2020, which may speak to the marketing angle of his various hot takes. By the way, you can book Dr. Makary for a speaking gig through his agency for $20,000-$39,999. He’s listed there first as a NY Times bestselling author, second as an NBC and Fox News commentator, third as a healthcare futurist, and, lastly, a surgeon then professor.
Interestingly, his agency bio describes him as a Professor of Health Policy, but again the Johns Hopkins Medicine website shows him as a Professor of Surgery. According to his Wikipedia page, he has a Masters in Public Health with a concentration in Health Policy from Harvard University. And he appears to have been associated with the Bloomberg School of Public Policy at some point, though he is not currently listed as a professor there. So he does appear to have some schooling on the topic of public health policy and presumably did some research and/or teaching on the subject in the past. Whether that had anything to do with global pandemic response could not be confirmed.
It should also be noted that Dr. Makary achieved some infamy earlier this year by predicting that America would reach herd immunity by April. Making fantastical predictions is a savvy way to garner headlines and I’m not one to begrudge smart marketing. And who among us hasn’t had a failed prediction or two? But instead of doing the reasonable thing by admitting that he was wrong, he has instead blamed the delta variant and everyone else for not understanding what herd immunity means.
I won’t attempt to decipher whatever nuance may exist when it comes to defining herd immunity, but here Dr. Makary sounds to me more like an agenda-driven politician refusing to admit wrong than a doctor in genuine pursuit of truth.
Another doctor, Mr. Jonathan Howard, wrote an excellent piece in response to Mr. Makary’s many wayward COVID takes that addresses the herd immunity topic (and others) much better than I ever could. By way of disclaimer, Dr. Howard is a neurologist, so consider his post a non-expert dismantling of a non-expert opinion. But he claims more than a passing interest in infectious diseases and has written a number of thoughtful takes on the subject of COVID.
In this day and age, fake experts are everywhere casting doubt on expert agreement, since “popularity and self promotion have replaced knowledge and experience as indicators of expertise.” Dr. Makary appears to fit squarely into this box. What is striking to me is how easily he inserts himself into a discussion that appears well beyond his purview, which I reckon results in a collective eye roll amongst his more informed colleagues. I wonder, for example, how he might respond if a virologist started opining on the usefulness of his surgeon checklist?
Ms. Weiss revealed her own bias by inviting someone with Dr. Makary’s track record on to her program. That bias was clear in how she engaged with Dr. Makary during their conversation as well as in the episode description, where she asks “whether we can safely — and finally — call time on the pandemic”, and says Dr. Makary “offers a no-nonsense approach” to the debate.
Dr. Makary has already failed once in calling time on the pandemic and there was plenty non-sensical about what he had to say.
…I will talk to infectious diseases doctors, they haven’t read the studies.
Dr. Makary followed his previous quote with this example of a logical fallacy known as hasty generalization, which is a claim based on a few examples rather than robust proof. It reminds me of a misappropriated aphorism about the plural of anecdote not being data. Dr. Makary is extrapolating a couple of personal observations that leads the listener to assume that most true experts on infectious diseases have for some reason decided not to read any of the COVID literature, therefore casting doubt on the legitimacy of all such research.
A couple of data points does not make a trend, and it strikes me as reasonably likely that his friends are more the exception than the rule. I have value investor friends who pay no attention to Berkshire Hathaway annual letters, but that doesn’t suggest to me that most value investors don’t read Warren Buffett’s musings. Epidemiologists avoiding studies on the greatest pandemic of their lifetimes is like astronomers ignoring research about an approaching asteroid with extinction-level potential. Just wouldn’t make much sense.
We have two pandemics: We have the COVID-19 pandemic and we have an accompanying second pandemic which is a pandemic of lunacy.
Dr. Makary points here to polling which found that a sizable segment of the population believes the risk of hospitalization with COVID is greater than 20%. He is likely referring to this Gallup survey and this chart in particular:
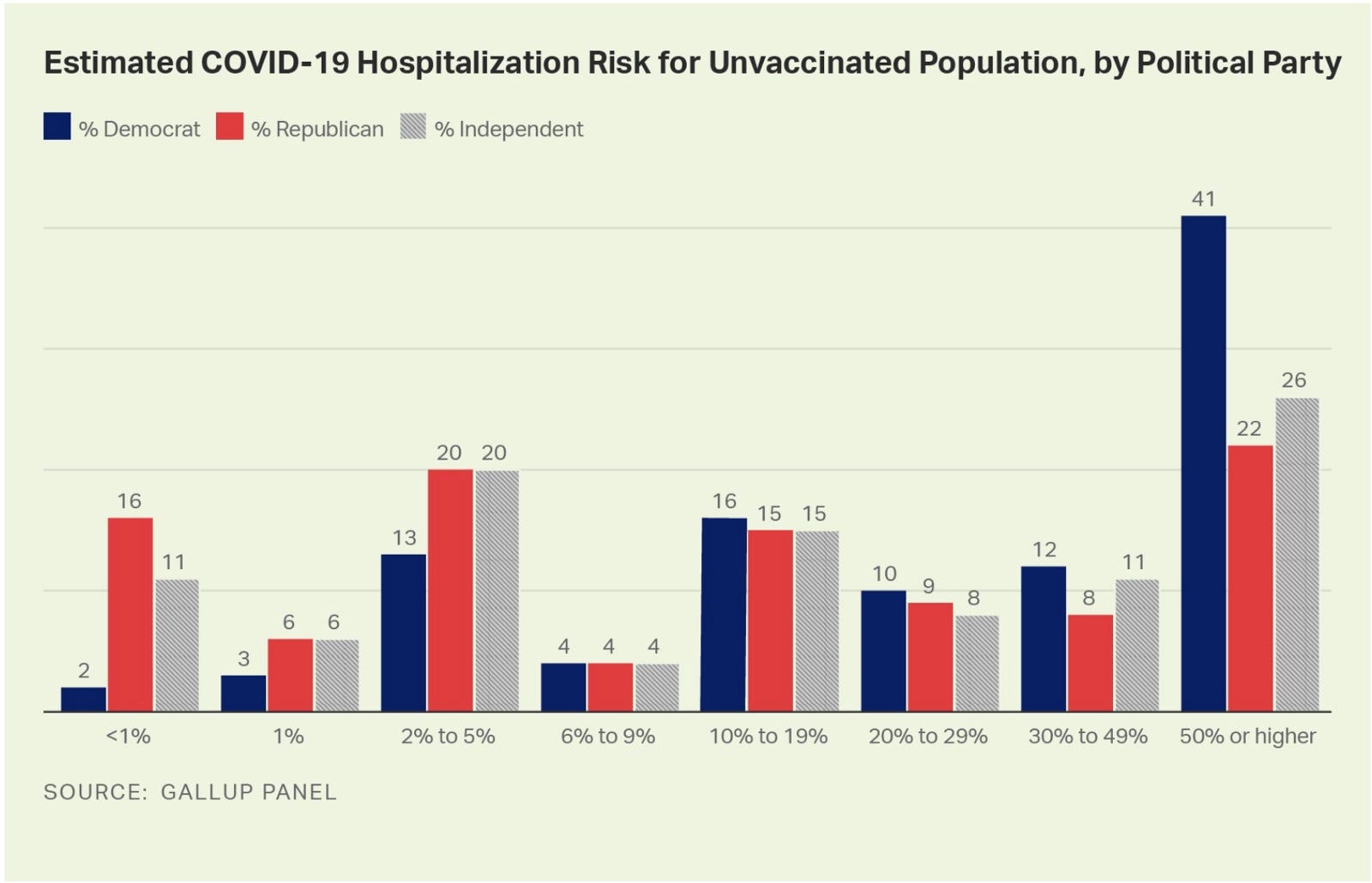
The bigger picture numbers are still wrong but not nearly as dramatic, which wouldn’t make for as fun of a talking point.
He later laments that “70% of people in this half of America belong to a political party — I won’t say which one because I stay out of politics — believe that the risk of hospitalization from COVID is over 20%. 41% believe that the risk of hospitalization is over 50%. It’s 1%.”
Dr. Makary’s presentation of this data is incorrect. To be more precise, 49% of Americans polled incorrectly pegged the risk of COVID hospitalization at over 20% (147/300). To comport to his own reading, 63% of Democrats (he rounded up to 70%) believe this to be true, which accounts for only 43% (63/147) of those “in this half of America” (not 70%). And it’s 61% (89/147) “in this half of America” that believe the risk of hospitalization is over 50%, 46% (41/89) of which is comprised of Democrats.
Putting aside his inaccurate portrayal of the data, a similar observation could have been made about Republicans, 54% of whom incorrectly believe the risk of hospitalization is over 10%. The magnitude of the misunderstanding is of course lower but the dynamic is the same directionally.
Misunderstanding of COVID risk should come as no surprise. Sadly, Americans believe lots of things that are factually incorrect. This in my view is a function of media bias and proliferation of non-expert opinion across social media platforms. This unfortunate reality was with us well before COVID, which just so happens to make for an easily contested flash point in our never-ending culture wars.
For example, 58% of Americans wrongly believe crime rates are higher today than they were 30 years ago. Why do we believe this? I suspect it’s because we live in a 24-hour news cycle that is desperate for clicks and can disseminate information instantaneously to billions of people across the world. If it bleeds it leads, and having such efficient access to crime reporting allows recency bias to misinform our collective perception of risk. Naturally (and sadly), there is a partisan element to these views as well: 54% of Democrats believe this “uptick” in crime is the result of loose gun laws compared to just 8% of Republicans who believe the same.
Another misperception that Dr. Makary could have highlighted is that 28% of Americans believe that the government is intentionally hiding the truth about the harmful effects of COVID vaccines. This also broke down along partisan lines, with just 9% of Biden supporters believing the same compared to 47% of Trump supporters.
Here’s another fun one: 20% of Americans believe COVID vaccines contain microchips as part of a government attempt at population control.
So which is more harmful to society at large: An overestimation of COVID hospitalization risk — where the downside is more vigilance — or belief that Bill Gates has brought Innerspace to life as part of some genocidal conspiracy — where the downside is entrenched paranoia and reduction in contagion mitigation efforts that only prolongs the pandemic?
The reality is that we as a society have long held misinformed views. This is a result of how and where people consume their news, whose delivery is almost always shaped by an agenda. The pandemic of lunacy Dr. Makary decries was with us well before COVID and will be with us long after. We did not suddenly lose our faculties when the virus arrived.
You must wear a mask in a restaurant for the nine steps until you get to your table and then you can take off the mask for two hours and yap and yell and talk and spit.
Here Dr. Makary ridicules the apparent illogic of wearing a mask in a restaurant only while not seated at a table, as if the act of mask removal during a meal negates any benefit of wearing the mask elsewhere. I would imagine that, while moving about a restaurant, the potential for entering an unknown person’s space increases dramatically when compared to sitting in one spot. Again, I’m no infectious disease expert, but my rudimentary understanding of spatial awareness suggests to me there may be wisdom in achieving some incremental protection when the surface area of engagement is increased beyond one’s intimate space. That is, I would presume it’s more likely that someone could contract COVID while walking by 20 random, unmasked people than they might when seated amongst a handful of known acquaintances (and interacting with a masked server).
Look at the farce of what’s happening…When you go to a gathering, the workers are wearing a mask and no one else is wearing a mask…We’re imposing a new form of oligarchy that is exercising a power imbalance that in any other setting would be seen as disgusting…Look and see who is wearing a mask, these are people from minority communities, low income poor people…who have to work during the pandemic and those of us who are enjoying cocktails, we’re told for you, you are dignified enough where your transmission is somehow sanctioned…and for other people it’s not.
You can almost see the picture Dr. Makary is referencing in his mind when he makes this statement. I‘d bet good money it was this year’s Met Gala, which saw the likes of Alexandria Ocasio-Cortez gallivanting around in fancy outfits while their handlers and servers were masked up. Plenty of points can be made about inequality with events like this, but the masking part of it misses the mark for me.

Firstly, Dr. Makary is making inaccurate generalizations about the service industry. A quick review of restaurant, banquet, and hotel worker demographics shows caucasians as typically the largest racial group, usually in line with census estimates (i.e., minorities are not disproportionately represented on balance). The split between women and men varies by role but on the whole breaks down roughly 50/50. So Dr. Makary is wrong to imply that the service worker community is minority-dominated.
Second, the power imbalance he describes would have to be ever-present for it to prove truly problematic in a discriminatory sense. But it is, in fact, only circumstantial. All of these service workers experience the other side of this perceived injustice during their off hours when they turn into the client. For example, the masked waiter at a fancy gathering is typically subjected to more liberal masking requirements when frequenting a restaurant on his own or grabbing a beer at his favorite bar.
These masking requirements derive from CDC and OSHA guidelines that define “medium risk employees [as] those who regularly come within six feet of other people, such as retail workers, restaurant servers and hair stylists.” Which is to say, the masking is as much designed to protect service workers as it is to protect gala attendees sipping their fancy cocktails. It stands to reason that those regularly interacting with a high volume of random people might want to take some extra precautions. This is a good example of the selective masking that Dr. Makary espouses when discussing whether he believes children should be masked in school.
Lastly, there are plenty of instances where the well-to-do are required to mask up. Indeed, we often see full, non-discriminatory mask enforcement when the numbers get large enough for indoor events. For example, fans are often required to wear a mask while attending NBA games. This rule applies equally to everyone, including those with expensive courtside seats. Even the players — with their multi-million dollar contracts — are required to be masked when not on the court. The same level of enforcement applies to patrons of the Chicago Symphony Orchestra, a demographic I presume ranks high on the socioeconomic scale. High fashion companies like Hermes and Louis Vuitton often require shoppers to mask up before entering their stores.
It is also worth noting that Met Gala attendees were required to provide proof of vaccination before attending. This seems an easier ask than requiring the same of all service workers, and I’m sure Dr. Makary would’ve complained about vaccine mandates that forced all employees to be inoculated in order to keep their jobs. Requiring masks instead of shots seems a reasonable compromise. Gala guests were also instructed to be masked at all times while indoors except when eating or drinking.
We have seen social inequality magnified during this pandemic through an oligarchy that has been telling this other group in the United States let them eat cake. Last year, we had a very healthy conversation…about racial equality in the wake of George Floyd…Fast forward just a couple months down the road and the vaccine comes out and guess what, people with power and influence insert themselves in the vaccine line. Board members, private jets flying to Florida…22-year old aestheticians in a dermatology clinic…basically saying in a societal way, our life matters more than those who are vulnerable and at risk.
Dr. Makary continues to beat the inequality drum here and does some pandering with his George Floyd comment. I’m not sure many would characterize the “conversation” we had following Mr. Floyd’s tragic death as “healthy”. Certainly not the 25 people who are estimated to have died during protests that resulted in over 14,000 arrests and billions of dollars in property damage.

People with power and influence always receive preferential treatment. This is nothing new. The fact that some of them gained early access to COVID vaccines should come as no surprise, nor did I see much handwringing about this fact. I’m not suggesting that inequality is wonderful for society, just that I don’t see how this instance magnified anything. I also found the 22-year old aesthetician to be an odd example, particularly given how specific he was with the description. When thinking about things that magnify inequality, 22-year old aestheticians getting early access to a vaccine would probably rate relatively low on the list of concerns for most.
What we’re doing now is using an indiscriminate mask policy at times when it may not even be working, and we don’t have any data that it’s working.
This statement was made in reference to the effectiveness of mask-wearing for children in school. Dr. Makary makes several authoritative assertions like this throughout the conversation. Any time I hear someone say we have zero data or evidence of something, I suspect hyperbole is at play. My standard course of action is to conduct a quick Google search to see what’s what. I’m not here to determine which interpretations might be the correct ones, but more to check whether the science is settled in such a way as to justify these types of emphatic statements.
The first thing that popped up was this Duke study that found masking of children to be effective. I also saw an interview with Dr. Nipunie Rajapakse, a pediatric infectious disease physician at the Mayo Clinic Children’s Center, in which she referenced “numerous studies” that found that masking children is not harmful and indeed provides significant protection.
But there were other articles that seemed to suggest otherwise. It would thusly appear that the science isn’t quite settled on this topic, making child masking appear not as cut-and-dry as Dr. Makary claims it to be.
If masks worked — and we have zero data on masks working — they would rank number six in mitigation strategies. Yet the entire culture wars are around masking kids.
As discussed, it does not appear to be settled science regarding the effectiveness of masking kids, so to say we have zero data is misleading. I couldn’t find anything referencing masking as number six in mitigation strategies. My understanding is that masking is indeed a low risk mitigation strategy, so this might very well be correct. But assigning a single subject as being the sole focus of today’s culture wars obviously makes no sense. Masking of kids likely ranks below many other hot button issues for the simple reason that not everyone has kids. In fact, only 40% of U.S. households contain children under the age of 18.
We have zero data on the risk [of COVID] to healthy kids. Zero.
Dr. Makary doubles down on zero to emphatically make a point that seems to be in dispute. Deaths among children are thankfully rare, but they do happen, even among healthy ones, and there is data on them.
“We know kids are less efficient transmitters.”
Another handy Google search surfaced multiple articles and studies suggesting that children are indeed efficient transmitters of the virus, with one Princeton study referring to them as superspreaders. There is also plenty of literature that agrees with Dr. Makary here. Seems the science is not quite settled on this topic, so here again we’re being guided by Dr. Makary’s binary reading of the literature.
Let’s be honest, there is a power imbalance going on. Schools were closed when bowling alleys were open. The absolute last group to reopen was gonna be schools. You know why? Because kids don’t vote.
This sounds like a clever talking point prima facie but loses its punch due to the simple fact that kids have parents who vote, many of whom have been terribly inconvenienced by school COVID protocols. In fact, this may have played a key role in Glenn Youngkin’s recent gubernatorial victory in Virginia. I appreciate the teacher’s union angle that Ms. Weiss brought up here, but I also suspect there is some wisdom in slow-playing anything related to kids since they are typically amongst the most vulnerable as a demographic.
If they do universal vaccine requirements, they will hurt kids that do not benefit from the vaccine. There will be unintended harm. Let me be very clear because the rate of myocarditis in adolescents was 1 in 7000 boys. Doesn’t sound very pretty. We’re talking about heart inflammation. Now, in the group of kids, when I say kids it’s really up to age 22, in the group of folks 15–22, one of those out of 100+, died. You talk about an indiscriminate vaccine policy for 72 million kids in America. By the way, Israel had a 22-year old death clearly from the vaccine…Israel s 1/38th the size of the United States. Are we prepared to extrapolate their deaths to our population of our young people.
This is one of the bigger misconceptions relayed by Dr. Makary during the conversation, and takes some time to disentangle.
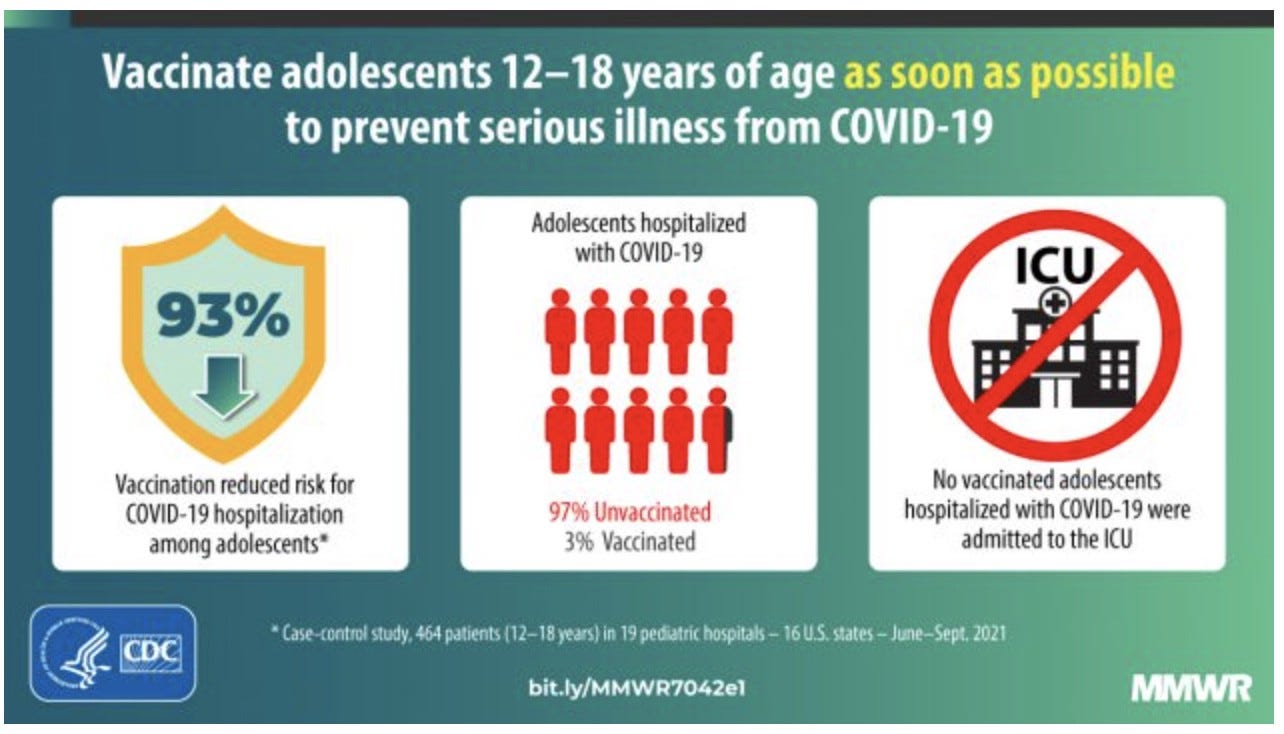
For starters, to claim that anyone — regardless of age — would not benefit from vaccines that have proven highly efficacious is obviously misplaced. He may be correct in suggesting only marginal benefit for young children — since they tend to be at lower risk individually — but to claim they would reap zero benefit appears incorrect. This has been proven in previous studies for adolescents in particular.
Second, Dr. Makary is mixing age cohorts here. He addresses the question of whether children (presumably in the 5–11 age cohort) should be required to be vaccinated by referencing what I presume are vaccine-induced myocarditis incidents in the older adolescent cohort. To his credit, Dr. Makary acknowledges the distinction, but I doubt most listeners will take the time to parse the data as presented. This distinction is important because, best I can tell, there have been no documented cases of children under the age of 12 dying as a result of being administered a COVID vaccine.
I’m not sure which study he is referencing but let’s run with the numbers anyway. Backing out the math, it would appear that there were approximately 700,000 adolescents (not children) studied in this trial (where 1 in 7,000 = 100 diagnosed). Of the 100 or so that were diagnosed with myocarditis, one of them died, which works out to a mortality rate of 1 in 700,000. Stated differently, adolescents stand a 99.999999% chance of not dying from myocarditis as a result of the vaccine. To put that in perspective, the odds of being struck by lightning in one’s lifetime are 1 in 15,300.
Of further note is that he mentions boys specifically. That’s because myocarditis tends to affect males at twice the rate of females. This would suggest that the study contained closer to 1.4 million adolescents (assuming boys and girls were equally represented). We can therefore roughly deduce that 1 in 14,000 females were affected, none of whom apparently died during the study (as surely Dr. Makary would’ve pointed that out). If my assumptions are correct, this would result in a vaccine-induced mortality rate among adolescents of just 1 in 1.4 million.
Dr. Makary has been publicly corrected on this framing before yet he continues to make these claims.
Israel has distributed 16.2 million doses of the COVID vaccine to its citizens, with roughly 5.5 million of them being fully vaccinated. To Dr. Makary’s point, there has been one reported death attributed to post-vaccine myocarditis. Those odds are even lower than the ones he used in the previous example, so the Israel experience only weakens his case.
Also missing is the average incidence of myocarditis ex-COVID. According to the Myocarditis Foundation, there were 3.1 million such cases globally in 2017. This is a condition that disproportionately affects males from puberty through their early 30s. The majority of cases are mild yet still resulted in 354,000 deaths in 2015, making it the third-leading cause of sudden death among children and young adults. Putting this in equivalent terms, myocarditis (ex-COVID) on average affects 1 in 2,548 people (out of 7.9 billion globally) with a case fatality rate of over 11%(!) in normal course.
Also missing here is an even higher incidence of myocarditis post-COVID infection. According to Yale Medicine, a study of college athletes found that 0.7% out of 3,018 COVID positive cases reported incidents of “cardiac involvement”. This is substantially higher than the 1 in 7,000 (.01%) risk Dr. Makary highlighted for post-vaccine myocarditis.
There are plenty of studies that disagree with Dr. Makary’s premise entirely, including from the American College of Cardiology and Harvard Medical School. Again, it’s not my place to determine which studies are correct. But I do believe it’s important to contextualize the data as presented by Dr. Makary, whose attempts at threat inflation are contested by many in the medical establishment.
[Natural immunity] protects you better than vaccinated immunity. It’s not perfect, but where are those cases of those who had COVID in the past and recovered, and are now intubated in the ICU or died. They’re exceptionally rare, and when they occur they’re in immunosuppressed or people with unique medical conditions.
Dr. Makary made this statement when asked by Ms. Weiss whether natural immunity can protect against COVID.
This is yet another authoritative proclamation about something that again appears to be unsettled science. Though he discounts what the CDC has to say about the topic, the consensus view among medical experts appears to disagree with Dr. Makary. Included in this group is Dr. Anna Durbin, an infectious disease expert and Professor of International Health at the Johns Hopkins Bloomberg School of Public Health and Johns Hopkins School of Medicine — as well as faculty member at the Center for Immunization Research.
Among other things, studies have indicated that over a third of COVID infections result in no protective antibodies and that natural immunity fades faster than vaccinated immunity.
Putting aside which studies and experts should be believed, doesn’t it stand to reason that the risk of vaccine-induced complications is smaller than the risk of COVID-related complications? As Dr. Durbin has noted, “Vaccines provide protection without any of the morbidities you can get with a natural COVID-19 protection.”
Vaccines also help stop the spread (at least pre-Omicron!), so I’m confused as to why Dr. Makary would appear to be advocating for natural immunity as a substitute for vaccinated immunity.
There are of course examples of people who have died after being infected with COVID more than once, though thankfully Dr. Makary is correct about the rarity of those incidents. You know what else is exceptionally rare? Vaccinated folks dying from COVID. And, as discussed, children and adolescents dying from vaccine-induced myocarditis.
If [someone] has had COVID, there’s no scientific evidence that they would benefit from the vaccine. That data does not exist.
This is another claim stated with such authoritative certainty that it begs further scrutiny. And we need look no further than Dr. Makary’s own school to find a contrary — and more informed — opinion. Dr. Lisa Maragakis, Senior Director of Infection Prevention, and Dr. Gabor Kelen, director of the Johns Hopkins Office of Critical Event Preparedness and Response, wrote an article that stated the exact opposite of Dr. Makary here. When posed the question of whether those with “natural immunity” still need a vaccine, the authors responded:
Yes, the COVID-19 vaccines are recommended, even if you had COVID-19. At present, evidence from Johns Hopkins Medicine and the U.S. Centers for Disease Control and Prevention (CDC) supports getting a COVID-19 vaccine as the best protection against getting COVID-19, whether you have already had the virus or not.
The authors go on to highlight various studies in support of this view. Dr. Makary may push back by claiming that the studies highlighted include those conducted by the CDC, which he says “would get disqualified in a 7th-grade science fair project”. Well, they seem good enough for his Johns Hopkins colleagues. So here again we’re left to assume that Dr. Makary’s reading of the literature is the correct one rather than those of actual experts on the topic. Whether his interpretation is right or wrong, to state that there is “no scientific evidence” and that the “data does not exist” is misleading.
As an aside, it’s fun to imagine the awkwardness when Dr. Makary encounters his Johns Hopkins colleagues who have dedicated their lives to the study of infectious diseases.

No one would ever act like this when there was influenza circulating in the community even though the case fatality rate is comparable.
This struck me as an odd thing to say on two levels. Firstly, we’ve known about the flu for many years and have learned to manage it through annual vaccinations and other remedies. Comparing the seasonal flu to a new and mutating virus struck my novice brain as nonsensical.
Second, is it really true that case fatality rates are the same? The CDC estimates that seasonal influenza kills about 36,000 people per year in the U.S. Meanwhile, we’re on track for nearly 800,000 COVID deaths in just the past two years. Granted, COVID is significantly more contagious than the flu, but surely not enough to account for such a large delta in the number of deaths.
According to Dr. Makary’s own university, the current case fatality rate of COVID is 1.6%. Most estimates I could find peg the case fatality rate for the seasonal flu at well below 1%, with several putting it at 0.1%.
Dr. Makary’s comments here appear to be demonstrably false.
They would never act like this with Coxsackievirus. Do you know there were as many kids with RSV in the hospital this year as there were with COVID? Didn’t get any attention…it’s not getting any headlines. They don’t give a rip that 400,000 kids died of malaria the year before COVID. Where’s the outrage? It’s such selective outrage.
Dr. Makary continues with the false equivalency here.
Coxsackievirus is better known as hand, foot and mouth disease. It is considered to be a relatively mild virus that impacts mostly children and usually resolves in 7–10 days. There is virtually no risk of mortality and only a small risk of hospitalization. Not quite the makings of a mutating virus with the potential to kill millions of people and cause a coordinated global shutdown.
RSV is a common respiratory ailment that usually causes mild, cold-like symptoms. It was discovered in 1956 and is recognized as among the most common causes of childhood illness. More severe cases lead to an average of 58,000 hospitalizations per year among children aged five or younger, making it the number one cause of pediatric hospitalizations year-after-year.
Firstly, why would a well-known disease with a rather predictable hospitalization rate steal headlines from an emergent virus that caused a global pandemic? Second, the numbers don’t add up. With 58,000 RSV-related hospitalizations per year, that averages out to 1,035 hospitalizations per week. According to a study conducted last summer, it is estimated that 0.4% of pediatric hospitalizations are due to COVID. With 5.3 million pediatric hospitalizations per year, that works out to 21,200 that are COVID-related, or 378 per week.
If there really were as many children hospitalized with COVID as there were with RSV at the time of this interview, that’s either a big problem (because the number of COVID admissions is higher than average) or it’s good news (because the number of RSV hospitalizations is lower than average).
According to the CDC, there were an estimated 409,000 deaths globally from malaria in 2019. Roughly two-thirds of those deaths tragically occurred in children under the age of five, which would equate to 274,000 kids. We’ll give Dr. Makary the benefit of the doubt with regard to the number of deaths, but to say that “they don’t give a rip” is not only vague (who is they?) but also disingenuous.
Funding for malaria control, prevention, and treatment totals billions of dollars per year. There are dozens if not hundreds of charitable organizations dedicated to fighting the disease, and celebrities routinely make it a focus of their philanthropic mix. A stated goal of the Bill and Melinda Gates Foundation is a “world free of malaria”. The Global Fund distributed 188 million mosquito nets in 2020 to help with prevention.
I don’t think any of this qualifies as “not giving a rip”. I can only assume he is complaining about the lack of malaria news coverage in comparison to COVID. But the reality is that we’ve known about malaria for over a century and it’s mostly a regional phenomenon at this point, so it’s understandable that it wouldn’t dominate global headlines amidst the largest pandemic of our lifetimes.
It’s pathetic to be honest with you because let’s assume COVID was eradicated, would the doctor have the same feeling about influenza? Guaranteed that doctor has never vaccinated their kid for influenza.
This was said in response to Ms. Weiss relaying the story of a doctor she follows on Twitter who said they would like to go to a store with their three-year old and not feel like they were risking the child’s life.
I agree that the story Ms. Weiss relayed is a pretty dramatic take. But here again Dr. Makary makes a false equivalence between two very different viruses. And his assumption about the vaccination status of that child is as unprofessional as it is unfounded.
Since Dr. Makary often extrapolates anecdotal data points, I’ll do so here myself. I am personally not nearly as concerned as this Twitter doctor appears to be when it comes to COVID, yet I have had my kids vaccinated against the seasonal flu each year that they’ve been eligible. I reckon if I’ve been willing to do so, then so too has this paranoid doctor.
The question is at what point do you let people ride a bike, and drive a car, and participate in sports, and go on a golf course, because there is a risk that a golf ball can hit you or that lightning could strike…let them make the choice, not us in public health.
Dr. Makary demonstrates a fundamental misunderstanding of group risk throughout the conversation, and this is a good example. Here he commits the same mistake many others do when it comes to the vaccine debate, which is allowing individual risk to inform broader risk metrics.
As the mathematician Mr. Nassim Taleb has explained, this represents a fallacy of aggregation. Lightning strikes, errant golf balls, and car accidents are not contagious. Thusly, the risk is not multiplicative like it is with a communicable disease. Per Mr. Taleb:
Under multiplicative events the risk for the collective do not scale up from the risks of an individual. Systemic risks can be extreme where the individual ones are low, or vice-versa…[for large enough groups] it is a tail risk/systemic problem computationally dissociated from the individual components.
What this speaks to is a micro versus macro dynamic that often goes missing in our COVID debates. So many people are focused on individual circumstances and less interested in understanding how personal decisions can impact those around them. My rudimentary understanding of viral replication is that suitable hosts are required in order to feed the beast. This makes the unvaccinated population ready vessels to facilitate propagation — and therefore mutation — of the virus. If you probabilistically decrease the number of hosts by way of vaccination, you hamper the ability of the virus to go forth and multiply, which should be expected to slowly choke out the danger and thusly reduce the number of COVID-related deaths over time. The type of individualist thinking Dr. Makary appears to endorse here is how the “minority threatens the majority” in moments like this.
It’s almost like the government is the arsenic and the firefighter. They’ve created the problem that they are there to solve with their own vaccine solution.
Funny flub to start this comment (arsonist, not arsenic). The primary problem to be solved for here is transmission of COVID. Lab leak likelihood aside, the U.S. government did not (at least directly or intentionally) create that problem. Nor is the vaccine the government’s solution since it was developed by private companies. As far as I can tell, the government has no economic interest in vaccine manufacturers and does not stand to directly benefit monetarily from their distribution. So the solution being advocated for by the government is not “their” solution at all.
And keep in mind the notion of incentives here: The government wants a happy and productive populace to ensure its survival, both by way of re-election and tax receipts. Whatever solution the government is endorsing will surely be in service of those overarching objectives.
No state will tell us who is showing up in the hospital except for one, North Dakota…The average age of a fully-vaccinated person going to the hospital — a breakthrough hospitalization — is 73. The average age of a breakthrough death is 80. So, what’s that tell ya?
What it tells Ms. Weiss is that we “should be even more enraged” that we are expected to wear masks two years into the pandemic.
It should be noted that the federal government has left mask guidance to the states, many of which have rather liberal masking policies. That said, it is well understood that COVID disproportionately affects the older among us. This makes sense as, similar to obesity, the elderly tend to be at higher risk for all sorts of ailments.
But just because COVID seems to be impacting mostly the elderly, does that mean the rest of us should not be inconvenienced to care? Mr. Taleb recently wrote a piece demonstrating the flaw in this thinking, first by making the point that “The main trait in civilized society is to protect the weak” and later with the following mental model:
Another problem…is that the way society is built is via dynamic not static reasoning. As I keep writing in the Incerto, a certain class of people…ignore that things move. A 30 y.o. is not going to be frozen in complete youth and (civilized) societies have been organized around intergenerational commitments: you treat the current elderly the way you would like to be treated when you grow older. For even [you] will be older some day…Why is it so difficult to grasp that by killing seniors, you reduce your own life expectancy?
The point he makes here is an important one. Not only does our vaccine hesitancy betray our collective civic duty in protecting the most vulnerable among us, but it increases the likelihood that similar intransigence will adversely impact us when the next pandemic arrives.
There is the notion of “long-term greedy” from the finance world that rings true here.
If you go on the CDC website and look at their guidance on the varicella chickenpox vaccine, it says we do not recommend the chickenpox vaccine if you have had chickenpox because you have long-term immunity.
This is more editorializing by Dr. Makary. He claims a negative affirmation in the form a specific recommendation by the CDC to not get the chickenpox vaccine, when in fact the guidance simply suggests that previously infected people “do not need” the vaccine. This is a subtle but important distinction given the difference in weight between actively recommending against a vaccine (which speaks to potential danger) versus simply saying it is not required (which speaks to necessity).
Also, chickenpox was discovered centuries ago, so I suspect we have a pretty good understanding of what long-term immunity might look like for something like that.
As many as 1 in 5 people in healthcare have left in the last two years. They’re leaving in droves and they’re about to leave in another mass exodus unless the court keeps the (vaccine mandate) stay on.
…40% of TSA were not fully vaccinated as of a few weeks ago. 22 fire stations in New York have closed…police officers all over the place are leaving with crime surging in Baltimore and other...
The healthcare resignations number looks to be accurate, but COVID vaccine mandates appear to have nothing to do with those resignations (at least thus far). The Atlantic conducted an analysis on what is behind the attrition and vaccine mandates were never mentioned. In fact, the primary reason for resignation is because these poor people are exhausted and overworked, largely thanks to wave upon wave of COVID patients.
Interestingly, the hospital staff turnover rate in 2019 was 17.8%, so maybe the 2020 numbers aren’t that dramatic all things considered. That could very well change, though a recent survey suggested that just 5% of unvaccinated workers have quit because of vaccine mandates. If this number holds for healthcare workers, then it should result in only a minor exodus. Thankfully, it appears TSA workers are tracking towards that number with a full 93% of them getting vaccinated by Thanksgiving.
The latest estimate of fire station closures due to mandate-induced shortages in NYC is a bit higher now at 26. This is obviously suboptimal. Not necessarily catastrophic in the context of NYC’s 1,667 fire stations but surely could have negative implications for local communities. I wonder how a former firefighter might feel about someone dying in their community because a fire was not put out in time?
There are indeed plenty of reports of police officers turning in their badges as a form of personal protest against vaccine mandates. The best data I could find on this was for the NYPD, which actually recorded very small numbers of resignations and suspensions related to the mandate. In fact, it looks like only 100 or so protesting officers were removed from duty out of a workforce 35,000 strong (0.3%).
It’s difficult to find updated total crime statistics for Baltimore. But there were less homicides in Baltimore in 2020 than in 2019, and the number of homicides this year is tracking less than last year. I know other cities (e.g., San Francisco) have seen a meaningful uptick in crime this year, but some attribute this more to the local philosophy of policing rather than number of police officers per se.
I think they got a taste of what it’s like to be king and they don’t want to turn the keys over.
Dr. Makary made this statement in response to a question from Ms. Weiss about “what’s in it for the oligarchy” when it comes to what the doctor believes to be overbearing and nonsensical COVID policy.
I appreciate the general sentiment about insular institutions being staffed by out-of-touch fuddy-duddies and run by power-hungry bureaucrats. But to ascribe power grab motivations to onerous COVID policies speaks more to Dr. Makary’s narrative bias than it does to the likely reality in my view.
This is where the idea of incentives comes into play. The CDC is incentivized by one thing, which is to mitigate as much as possible the risk associated with COVID. Social, political, and economic implications probably don’t factor much into its analysis because those issues are beyond its purview. Its focus is therefore singular in nature: stop the spread of COVID while leaving political and financial implications for other authorities to navigate.
A creeping sense of zeroism naturally sets in when the objective is to mitigate downside rather than maximize upside. Put another way, the CDC is heralded for bringing about an end to the pandemic but not necessarily rewarded for doing so in as gentle a manner as possible.
Politicians, on the other hand, are focused on the acquisition, maintenance, and projection of power. Dr. Makary seems to suggest they are using COVID policy to exercise the projection part of that power equation. But this misses the larger objective of most politicians, which is to get in office and stay in office. Antagonizing one’s voter base with restrictive policies that inhibit economic production and impinge upon individual freedoms probably isn’t a recipe for success.
I would imagine a win for everyone here is to get this whole thing over with as quickly as possible with the least amount of collateral damage, not to prolong it for control purposes.
When HIV hit this country, Dr. Fauci immediately started talking incessantly about a vaccine that would bail us out of the HIV epidemic. Guess what? We never got a vaccine. It was therapeutics…that allowed us to manage the infection. Same here. An intense focus on vaccines, which we needed…but there are so many therapeutics now…
This was an odd analogy to make since it sounds like Dr. Makary is making the case for therapeutics over the vaccine. Comparing our HIV response to COVID makes little sense given that we’ve developed a vaccine for the latter and not the former. So it’s not the “same here”. For someone who says he’s pro-vaccine, he makes a lot of statements like this that suggest otherwise.
Fluvaxomine, which is Prozac, reduced hospitalizations by 91%. A German study just came and said that almost no one died with high levels of vitamin D in a meta analysis. Hypertonic saline, a nasal spray you can buy for $4 over the counter reduced your hospitalization risk from 10% to 1.2%. Steroid nebulizers, actively included in standard of care in the UK, not even acknowledged here.
A couple of new studies have indeed shown that fluvaxomine may be an effective therapeutic for COVID. It appears Dr. Makary got his numbers mixed up, but it is nonetheless great news and he’s right on the trajectory at least.
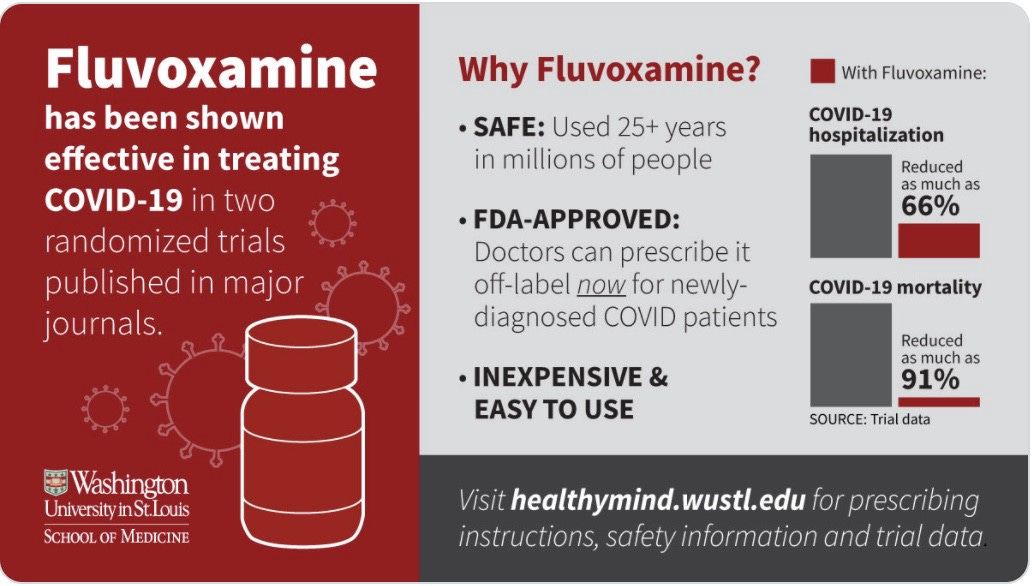
However, it’s important to note that these studies are new and have not yet been peer reviewed. In fact, a number of experts have already contested the findings, so I guess we’ll have to see how this shakes out.
Pending validation aside, do you know what has proven even more effective at reducing hospitalizations and deaths? You guessed it: The COVID vaccines!
I wasn’t able to find anything to confirm his stats on the effectiveness of hypertonic saline nasal sprays, but I did come across a few studies that seemed to indicate positive findings.
What stood out to me with the fluvaxomine and nasal spray studies is that they didn’t appear especially robust (e.g., the fluvaxomine study included only 1,497 people, half of whom were given a placebo). Dr. Makary expressed reticence previously in extrapolating vaccine data for just 1,500 kids but seems fine extrapolating small data sets when they conform to his narrative.
I couldn’t find the German vitamin D analysis Dr. Makary referenced, but there are a number of studies that suggest vitamin D deficiency may be a driver of COVID outcomes. But there seems to be plenty of disagreement here amongst the scientific community, so again this appears to be a contested assertion.
From what I could find, steroid nebulizers are inhaled steroid treatments usually designed for asthma patients. It appears that this form of COVID treatment has not been approved by the WHO or CDC. And judging from official NHS communications — which specifically stated that “there was no statistically significant improvement in COVID-19-related hospitalisation or deaths” and that “inhaled budesonide is not being recommended for routine use” — it doesn’t sound like nebulizers are part of U.K. standard care.
But there do appear to be studies suggesting at least some benefit to them. So here again we have Dr. Makary making unsettled science sound more settled than it really is.
With this rant, Dr. Makary makes it sound as if the FDA has not approved any therapeutics, which is incorrect. The FDA has approved remdesivir and has granted Emergency Use Authorization for the monoclonal antibody treatment REGEN-COV. It’s just that the FDA hasn’t approved all the other things Dr. Makary appears to like. At least not yet.
In any other industry, if you’re this wrong you would no longer hold your job. It’s sad, when I read the studies…even Pfizer’s new drug, the pill, the oral pill, the 5-day pill, cut COVID deaths to zero. One of the main components, Ritonavir, that’s been around for decades. Why weren’t we doing those trials last year?
This is yet another odd criticism. It’s like asking why Apple didn’t release the iPhone in 2006 instead of 2007. I mean, all the parts were there for the company to make it, right? Why couldn’t they just figure it out earlier?!
Perhaps he’s criticizing Pfizer for focusing on the vaccine before the pill. But it strikes me as logical that prophylactics would be prioritized since the goal should be slowing transmission as quickly as possible. Then we can take on therapeutics as part of ongoing treatment needed for inevitable breakthrough cases. Makes sense to me to start with prevention then move to treatment. That way you can mitigate propagation of a virus that has an insatiable desire to replicate. But again, I’m no expert…
One thing I do know is that talking heads are wrong all the time. Yet they continue to get invited back for more of their misplaced punditry, so long as it adheres to whatever narrative is being pushed by the host outlet.
We’ve completely ignored the fact that the reason we have one of the highest death rates in the world is we have one of the most obese populations in the world. We’ve completely ignored comorbidity in data. That’s how I think we got into this problem.
…the number one risk factor for COVID…is the metabolic syndrome from obesity.
I don’t see comorbidities being ignored anywhere. I’ve personally heard it mentioned over and over again. Another handy Google search pulls up lots of results on the topic. And a list of comorbidities is provided on the CDC website that includes obesity, where it specifically states that “people with certain medical conditions…are more likely to get severely ill from COVID-19”. The CDC also published a study earlier this year which found that 78% of COVID-related hospitalizations were among the overweight and obese, with similar numbers for intensive care, medical ventilations, and death.
Though a recent Columbia University study suggested that comorbidities had no predictive power in determining COVID outcomes, it stands to reason that obesity would increase the risks associated with COVID since it increases the risk with all sorts of ailments.
But the correlation between obesity and COVID mortality isn’t as straightforward as Dr. Makary makes it seem since it doesn’t hold across countries. The U.S. is the 12th-most obese nation in the world and, per Johns Hopkins, ranks 20th in COVID mortality (measured as deaths per 100,000). Most of the countries ahead of the U.S. in obesity are tiny island nations nicely sequestered from the rest of the world, so their COVID incidence has been de minimis.
Kuwait, however, ranks 11th in obesity and 93rd in COVID mortality. Jordan ranks 13th in obesity and 65th in COVID mortality. Saudi Arabia ranks 14th in obesity and 113th in COVID mortality. Qatar ranks 15th in obesity and 117th in COVID mortality. Our neighbors to the north, rank 26th in obesity and 82nd in COVID mortality. Mexico ranks 29th in obesity and 23rd in COVID mortality.
But let’s assume anyway that obesity is America’s primary problem when it comes to combating COVID. What are we supposed to do with that? It has proven difficult enough to get people to incur the minor annoyance of wearing a face mask or submit to a couple of free shots. How easy might it be to convince a population of stubbornly entrenched habits to meaningfully change their lifestyles? Even if we were to miraculously convince everyone to get fitter, it would take years for those changes to reflect in broader society. What good does that do for a mutating danger present in the here and now?
Imagine our country undergoes a massive cyberattack that cuts off everyone’s access to the internet. The only solution is for folks to individually code their way out of it or install free antivirus software created by Google, Apple and Microsoft. Which is more productive in addressing the immediate problem: Downloading that free software or suggesting that more Americans learn how to code?
Shouldn’t the message be to get the shot to assist with mitigating the immediate crisis AND maybe cut back on those carbs and get some cardio in?
By the way, Johns Hopkins does not list obesity as a major risk factor for COVID. It appears from their list that old age is the number one risk factor, followed by heart disease, lung disease, and diabetes (which presumably has an obesity link).
Natural immunity threatens the message that we need to vaccinate every human being with two feet. The message is ‘Hey, how dare you do that? People might go out there and choose to get natural immunity, that is choose to get the infection instead of get vaccinated. And we cannot allow that to happen’. So you’re saying we can’t be honest with people? We can both be honest about natural immunity and its effectiveness and encourage people to get the vaccine at the same time.
I agree we should be honest with people, both in acknowledging the limitations and morbidities associated with natural immunity, and in quantifying the societal damage such a pursuit might cause.
There are approximately 256 million adults in America. According to FiveThirtyEight, 30% of them are unvaccinated, which equates to 77 million people. The CDC estimates that roughly one-third of Americans have already had COVID, which would mean that there are 52 million American adults walking around with neither vaccinated nor natural immunity.
Some experts suggest that everyone will contract COVID at some point, but let’s be conservative here and estimate that only 25 million of those non-immune adults eventually catch it. Per the Gallup study that Dr. Makary referenced several times, it is estimated that the COVID hospitalization rate is between 1–5%, so let’s split the difference and call it 3%. And the latest COVID fatality rate in America is approximately 1.6%.
Using the above data, the expected net result of folks choosing natural immunity would be an additional 750,000 hospitalizations and another 400,000 projected deaths. For reference, there have been 3.5 million COVID hospitalizations to date and about 791,000 deaths.
Even if forthcoming therapeutics cut those numbers in half, we would still be inviting significant numbers of unnecessary deaths by suggesting that people should choose natural immunity over vaccinated immunity.
I sometimes think we would’ve done better in the pandemic if we didn’t have the CDC. Because the CDC consistently put out unreliable recommendations and we can’t have a group of disconnected people adjudicating on every aspect of American life.
Dr. Makary made this statement when Ms. Weiss asked whether he trusts the CDC. For starters, the CDC obviously doesn’t seek to adjudicate on “every aspect of American life”. This is yet another example of the hyperbole he often uses for dramatic effect.
He also has a striking amount of impatience when it comes to the CDC. A more liberal interpretation of the agency’s changing recommendations might be that it is trying to adapt in real time to a rapidly evolving situation. Dr. Makary admitted that he backed the early lockdowns because we didn’t know what we were dealing with. We certainly know much more today than we did then, but the situation remains fluid, as we can see with these new variants. I would expect guidance to remain fluid as well, especially as new research comes to light.
And since “we can’t have a group of disconnected people adjudicating” on our lives, I reckon Dr. Makary doesn’t have much love for Congress or the Supreme Court either.
Some women are reporting menstrual irregularities with the vaccine. There is something going on…
There have been reports of menstrual irregularities post-COVID as well. And there are theories as to why this may be happening. Bottom line is that there are no systemic studies yet on this phenomenon, so it might be more appropriate for Dr. Makary to say there might be something going on rather than there is something going on. This appears to be further evidence of premature certainty on the part of Dr. Makary.
People should be able to make their own decisions and if they’ve chosen not to get vaccinated, they have done so at their own individual risk. They pose no risk to those who have immunity…
Dr. Makary is again committing the miscalculation error of micro versus macro risk.
Ms. Weiss then asked if there are “30 people sitting around a Thanksgiving table and 29 have been vaccinated and one isn’t, those 29 people are protected from that one person.”
…That’s right. I mean they have a risk of, let’s say they’re under age 50 with no comorbidity, of being hospitalized of maybe 1 in 100,000. Now is that a risk that is acceptable? I would think so. Because if you drive to get a vaccine, you have a greater risk of dying on the ride to get vaccinated.
Dr. Makary often laments our collective misunderstanding of risk when complaining about COVID policy, but he makes the same mistake multiple times himself. This recalls for me Mr. Taleb’s description of the Intellectual Yet Idiot given “his misunderstanding of probability theory and cosmetic use of first-order models.”
Here Dr. Makary is conflating the lifetime risk of death due to automobile accidents with per incident risk, which is incorrect framing. Assuming one is driving a car (rather than motorcycle), the lifetime odds of dying in a car accident are 1 in 608. The odds of dying in a given year are 1 in 47,852. But with this statement, Dr. Makary is referencing very specifically the risk of death while driving to a singular destination.
Americans drive 3 trillion miles per year. There is an average of 7,000 car occupant deaths per year. That works out to 1 death per 428 million miles driven. Assuming a trip to the local pharmacy is within ten miles, the odds of one dying while driving to get a COVID vaccine are infinitesimal, and orders of magnitude lower than 1 in 100,000.
Putting aside his clear miscalculation of incidental risk, I find it interesting that he considers a 1 in 100,000 risk level acceptable in this context while a 1 in 700,000 risk of vaccine-induced myocarditis death among adolescent boys is unacceptable.
Senior advisors to the White House have said, people who are unvaccinated should get tested twice a day at their own individual expense in perpetuity. That is not medicine, that’s political vindictiveness.
I could find no confirmation that senior advisors to the White House have suggested that unvaccinated people take COVID tests twice per day. Even if they did, no such policy exists because that would obviously be ridiculous.
It is true that unvaccinated federal employees must submit to weekly or bi-weekly testing, but to peg that frequency at twice a day is incorrect. Unvaccinated visitors to the White House are required to be tested and to foot their own testing bills, but staffers see their testing costs borne by taxpayers.
Second, there is no realistic basis to assume any of this will persist “in perpetuity”.
Lastly, politics have nothing to do with policy implementation here. That is, there is no political test associated with testing requirements. Vaccination status may indeed correlate with political affiliation, but party loyalty has nothing to do with whether anyone needs to be tested. The determinant variable here is not whether someone is Democrat or Republican but rather whether they are vaccinated or unvaccinated.
COVID has become so stigmatized that doctors have actually refused to do transplant operations if someone, say, has natural immunity but they haven’t gotten vaccinated. OK so, are we gonna stop taking care of people who eat too many potato chips? Or people who have HIV? Or people who broke a bone in the past from being a BMX racer? And they come back with another broken bone? Are we gonna say, there were risks out there and you failed to listen to our guidance and therefore we’re not gonna take care of you? People have lost their minds.
I’ve no idea whether refusal to conduct transplant operations is a moral or medical quandary, but this more false equivalency since obesity and broken bones are not contagious. And HIV is not nearly as transmissable as COVID (and isn’t killing nearly as many people or causing the global economy to come to a screeching halt).
No one’s talking about Sweden right now. Sweden’s doing the best in the world.
Dr. Makary seems to agree with a view that is common amongst policy antagonists, which is that the relatively hands-off Swedish model is a viable alternative approach to COVID.
Sweden is a lovely place. I’m sure it’s the best at many things. It apparently ranks best in the world for sustainable tourism and is ranked #9 in the US News and World Report Best Countries report.
On COVID policy and outcomes, though, not so much.
Despite Dr. Makary’s claim, there are plenty of people talking about Sweden these days when it comes to COVID, and not for reasons he implies. Another handy Google search picks up multiple headlines about Sweden imposing new COVID restrictions as cases rise, offering booster shots, and introducing vaccine passports for indoor events.
Why would that be the case if Sweden is “doing the best in the world”? Could it be because Sweden’s COVID case and mortality rate has been dramatically higher than its Scandinavian neighbors? Could it be because it was determined that the country acted too slowly in handling the pandemic?
The reality is that the Swedish model hasn’t been the smashing success that many pundits claim it to be. The country has experienced 10x as many deaths per capita as its Nordic neighbors and hasn’t fared much better economically.
So here again Dr. Makary’s comments appear to be misleading.
We told people that indoors was better than outdoors. We got it backwards. We told people that vaccinated immunity is better than natural immunity. We got it backwards. We told people to wash their hands like crazy for 20 seconds. Stop at 15 seconds, you feel guilty…We made so many mistakes.
I don’t recall any specific guidance that suggested indoor activities were recommended over outdoor activities. Dr. Makary may be referring to the early days of the pandemic, when everyone was instructed to stay home during lockdowns (which he claims to have supported), but the benefits of being outdoors seems to have been clear for some time now.
As previously discussed, the notion that natural immunity is better than vaccinated immunity is heavily disputed.
I also find it odd that a doctor would seem to suggest that washing one’s hands is unnecessary when combating the spread of anything, aerosol or otherwise. UNICEF continues to recommend that children wash their hands, for reasons that appear axiomatic:
Respiratory viruses like coronavirus disease (COVID-19) spread when mucus or droplets containing the virus get into your body through your eyes, nose or throat. Often, the virus can easily spread from one person to the next via hands. During a global pandemic, one of the cheapest, easiest, and most important ways to prevent the spread of a virus is to wash your hands frequently with soap and water.
And I’m going to go out on a limb here and bet that there isn’t a single person on the planet who has ever felt guilty for only washing their hands for 15 seconds!
In Conclusion
As a free speech diehard, I have no problem conceptually with Ms. Weiss featuring the likes of Dr. Makary on her podcast. I share a suspicion of all things establishment and, frankly, believe our elected leaders represent the worst of our society intellectually and ethically (especially our modern vintage). I therefore sympathize with the general thrust of these types of discussions.
I do, however, have more faith in our scientific institutions, especially when it comes to things like the actual saving of lives. It is here that the government is called upon to perform the function of “tail risk manager”. I therefore find it unfortunate that: 1) Dr. Makary has staked the claim he has in the COVID debate; and 2) Ms. Weiss did not challenge even the most obvious mistruths (e.g., Is there really zero data for all these things?).
I believe the information Dr. Makary is disseminating is providing fuel for the vaccine hesitant among us, which may only work to prolong this crisis. For example, the aforementioned Dr. Howard recently posted another piece asking the question of whether contrarian claims about the pandemic’s end actually resulted in a false sense of security that had the paradoxical effect of extending the pandemic.
I don’t mean to suggest any ill intent on the part of Dr. Makary. I can only assume his views are genuinely held and surely he wants as many lives spared as possible in this whole thing. I just think his views are misplaced and counterproductive, especially in how he presents them by often using inaccurate and non-contextual framing.
Something to ponder with the likes of Dr. Makary, who certainly is not alone as a medical professional speaking out against COVID policies, is that those doctors most vocal in their views tend to be furthest away from the front lines. Indeed, it’s not often you read about a doctor who actually treats COVID patients making the types of claims that we heard in this podcast. Quoting Mr. Taleb again:
The error continues because someone else is paying the price.
I ultimately view vaccines as the least of all evils, likely doing way more good than harm in the grand scheme. For those expressing hesitancy because we don’t know the long-term effects of the vaccines, I again reference the work of Mr. Taleb, who has suggested that meaningful morbidities associated with vaccines would’ve shown by now given the massive number of vaccinations that have already occurred.
For those who point out that vaccine manufacturers still qualify for legal immunity, so surely something may be afoot, I employ a little common sense. If these companies knew that their vaccines stood any meaningful chance of sickening or, worse yet, killing their customers — which now count in the billions — surely that would be bad for business, no? Legalities aside, the existential risk remains the same for these companies.
Then there is the micro versus macro risk that I’ve already discussed. I have personally been boosted, not because I’m overly-concerned about my own risk but because I feel compelled to protect those around me by doing my part to stop the spread and reduce the strain on our hospitals. This is a form of civic, almost patriotic duty that I feel. It saddens me that so much of our country is so caught up in the politicization of it all that they allow their individual interests — however misplaced — to rule over the interests of their fellow citizens. This is a selfish stance in my opinion, and ironically predominant amongst those whose political affiliations are historically associated with the more “patriotic” of our political parties.
I cannot imagine how this generation of Americans would respond to the call to storm the beaches of Normandy when they can’t even muster a few shots to help prevent more deaths in their own families and communities.
Thankfully, Sam Harris dropped a COVID-focused podcast episode of his own just as I finished writing this piece. In it, he injects some sanity into the debate by interviewing an actual expert on these issues, Dr. Nicholas Christakis, a sociologist and physician with expertise in biosocial science. I can’t help but think that Mr. Harris felt compelled to have this discussion after listening to the conversation between Ms. Weiss and Dr. Makary. To which I say, thank you Sam!